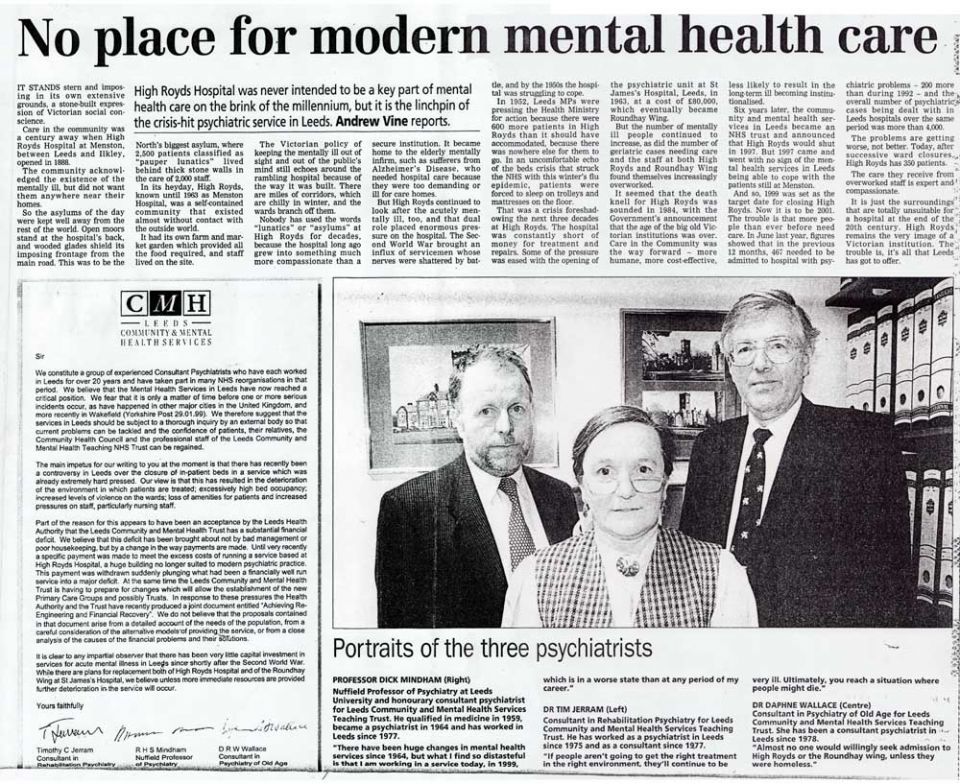
Professor Richard Mindham worked at Menston hospital from 1977 to his retirement in 2000. In 1977 he was appointed to the University of Leeds as Nuffield Professor of Psychiatry with the remit of setting up the 'Professorial Unit' at HRH.
For the first ten years or so the unit was accommodated in the Escroft Block which is the 'Modernist' building second on the left entering the hospital by the main entrance. Later due to the structural faults in that building and the general contraction in the hospital the team moved to the 'Admission' block which was the first major building to the left of the Administrative building. The professorial unit provided part of the psychiatric service to the western part of Leeds. One of Dr. Mindham's colleagues from the start was Dr Tim Jerram who still lives in the area.
After he retired Richard took up his long-standing interest in architecture more seriously and joined a course run by the University of Leeds. For his dissertation he undertook a study of mental hospital architecture entitled 'The influence of clinical factors on the design of hospitals for the mentally ill.' This included a substantial study of the architecture of HRH but his aim was to place its design in a more general context rather than to study it in detail. Richard describes High Royds "as a fine building and very well executed by Whittaker Bros. It was in many ways the ultimate in mental hospital design.
I was intrigued by the new buildings of 1938 which are of great architectural interest; a fact which I had not fully appreciated when I was working in one of them!" For some time now he has been communicating with Leeds Civic Trust over the fixing of a plaque to draw public attention to the buildings importance.
An extract of his dissertation on the architecture is published below with the kind permission of Professor Mindham. The full text can be accessed through the Library of the University of Leeds, School of Fine Art, History of Art and Cultural Studies,Centre for Architecture and Material Culture.
The West Riding Pauper Lunatic Asylum at Menston shows how the Board responded to its experiences at Wakefield and represents the most advanced design of hospitals for pauper lunatics. For this reason I have chosen it from among the West Riding Asylums to be described in some detail and to relate its layout to the themes which have emerged in the designs of Bethlem Royal Hospital and the Wakefield Asylum.
Early mental hospitals had suffered from a series of problems in conducting their work many of which could be attributed to the inadequate design of their premises.
The requirements which had emerged included: a need for the separation of the sexes, suppression of noise, ventilation, heating, delivery of supplies and disposal of waste, separation of patients on the basis of diagnosis or degree of disturbance, observation of patients and supervision of staff, accommodation of patients who failed to improve, provision of occupation for patients, segregation and care of the physically ill, security of patients, staff and hospital property. However it was the provision of a humane system of care for large numbers of people in the absence of means for effecting cures of mental illness which provided the greatest challenge.
In the last quarter of the nineteenth century the mental hospital had to provide facilities for the care of mentally ill patients at all stages of their illnesses. Initially they had to care for the acutely ill. This required accommodation which could provide a secure environment for disturbed and vulnerable patients with arrangements which protected patients, relatives and staff from harm and at the same time allow such treatments as were available to be effectively applied. After the acute stage of an illness patients required a regimen which could prepare them for ordinary life after discharge from hospital. This required the provision of facilities for rehabilitation. A substantial proportion of those admitted did not recover sufficiently for them to return to a normal life outside hospital and this led to an ever-increasing need for accommodation of patients who resided in the hospital indefinitely. The long-stay patients needed occupation as well as accommodation and their needs had a major influence on the siting, design and construction of county mental hospitals. All of these needs had to be met within the budget.
The design of High Royds Hospital [HRH] demonstrates how many of these demands were met. The hospital was essentially two hospitals, one for men and one for women, each being a mirror image of the other. This allowed segregation of the sexes including both patients and staff: only the most senior staff worked on both sides of the hospital.
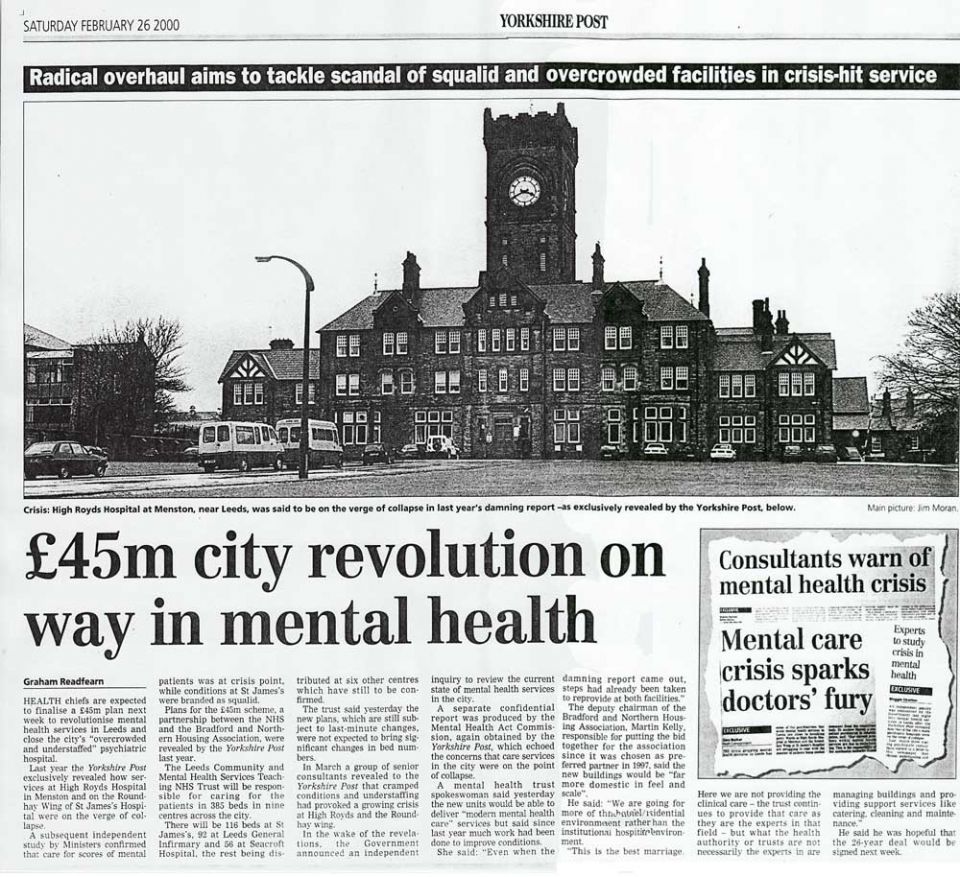
The pavilion model was adopted for the wards which allowed segregation of patients with different conditions or clinical requirements. This layout also had advantages reducing the likelihood of cross-infection and reduced the transmission of noise between the wards. The hospital was built on the echelon plan with the administration and residential accommodation for staff at the apex of the triangle, the wards stretching backwards on each side, one male, one female, and the supporting services set behind the administrative block. The individual buildings were joined together by a v-shaped corridor with some connecting corridors. The administrative block was surmounted by a massive tower which held a water tank and carried a clock visible all over the grounds.
The clock was controlled by a master-clock which also governed repeater clocks all over the hospital. This was perhaps, an indication of how the hospital was to be administered. A particular advantage of the echelon plan here is that the wards mostly enjoy a southerly aspect with extensive views over gardens and of open country. Patients admitted acutely to the hospital were initially observed and treated in wards close to the administrative block on each side unless they had special requirements on account of exceptional disturbance, infectious diseases or age. At HRH the wards immediately adjacent to the administrative block and those closest to the resident medical officer’s quarters were those for the elderly and frail. The wards for the newly admitted were placed next in the corridor.
After some weeks or months of treatment in the admission blocks patients might be discharged, transferred to a rehabilitation ward or admitted to a long - stay ward. The long stay- wards were further away from the centre and in some cases detached from the main hospital corridor system. There were special wards for epileptic patients and those suffering from the late effects of venereal diseases. In the nineteenth century there were no effective anti-convulsive drugs so that many patients were admitted to mental hospitals for care. Many of those who suffered from syphilis had the form known as dementia paralytica in which there are both problems in movement and impairment of intellectual functions which required distinct methods of management.
An important feature of the later mental hospitals, including HRH, was that there was provision for the separate care of the physically ill. At HRH the "infirmary wards' were at the back of the hospital to the north beyond the boiler house and well away from the other wards. Tuberculosis was a particular problem in institutions where large numbers of people lived and slept in close contact. Tuberculosis is infectious but is not usually acquired by casual contact; transmission requires close and regular contact with people who may be susceptible though other adverse circumstances such as poor diet and general ill- health. The conditions of a large mental hospital made tuberculosis a regular problem.
As the operation of the hospital was originally conceived patients formed an important element in the hospital workforce and this was seen to be therapeutic and desirable. They were employed on the farm, in the gardens, in all the domestic departments including the kitchen, bakery, laundry, cobbler’s shop. tailor's shop, plumber's shop, carpenter's shop, paint shop, hairdressers and library. These forms of employment were seen as fitting to their previous stations in life. As time went by specific occupational facilities were developed as part of rehabilitation. This included an occupational therapy department which used handicrafts for stimulating activity, a readiness for a return to tasks at home, and social interaction. Later an industrial therapy department with special workshops which simulated the working environment of the district was established allow to patients to participate in their former work. Each required special accommodation.
The heating of the hospital was initially by coal fires which were fed by gangs of patients who moved around the hospital throughout the day. Later central heating was introduced and this was initially fired by coal but later by other fuels. During the erection of the hospital a railway branch-line had been constructed to carry building materials and this was retained for the delivery of coal and other supplies. Ventilation was achieved by individual shafts for each ward that led to ventilation towers in each of the pavilions. These form a striking architectural feature of the hospital. The hospital has its own water supply which was initially stored in cisterns before distribution from the tank in the central tower.
The hospital was connected to the public sewer. Lighting was initially by gas but this was later converted to electric power.
All the doors in the hospital had locks that were part of a coordinated system of security and could be opened by a single key.
The type of key which was issued to a member of staff depended on their seniority, the Medical Superintendent and the Matron had 'Grand Master' keys giving access to all parts of the hospital; staff at others levels in the hierarchy had keys giving access only to those parts of the hospital in which they worked ; patients did not have keys. The design of the wards was very different from those at Wakefield or at Bethlem. All those subjects who did not require a separate room for clinical reasons were accommodated in large wards. Dormitories holding as many as a hundred people were used for the chronic wards and even the admission wards.
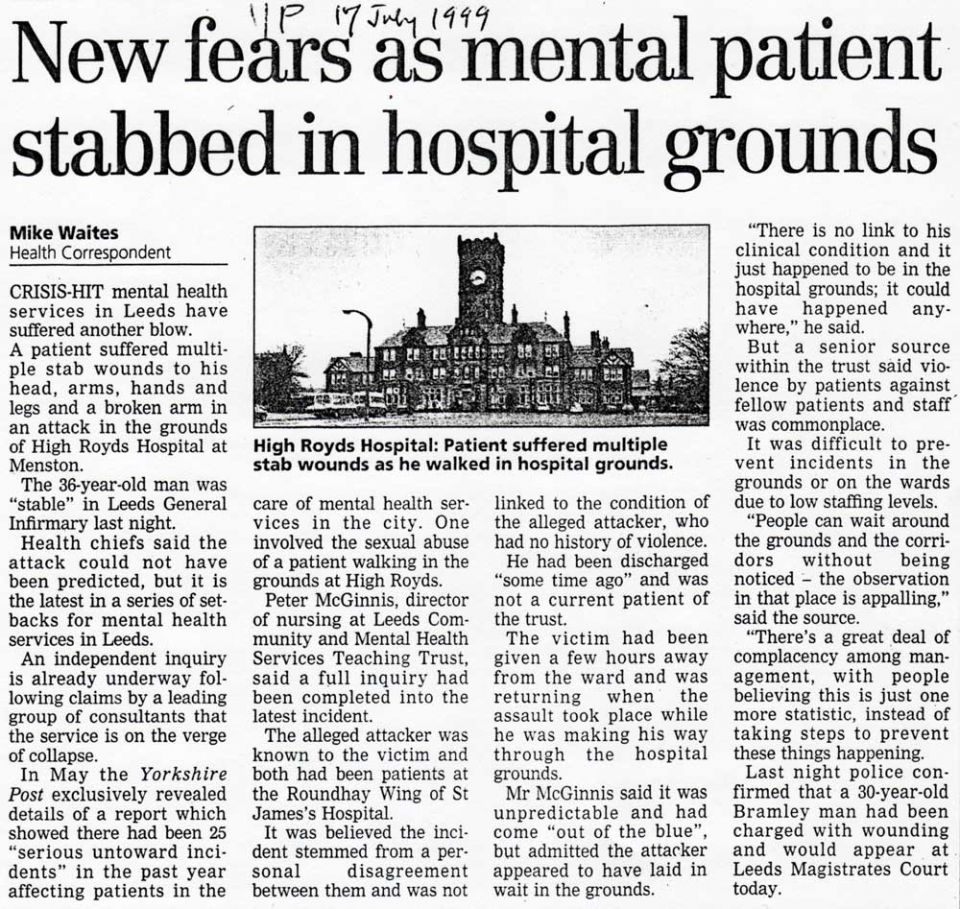
Approaching the hospital from the main entrance one is impressed by the scale of the building and its landscaped grounds. The central tower, with its clock, dominates the front of the building. There are extensive buildings to each side and others which stretch behind. The building is constructed of local stone which has weathered with age. There are three levels of decoration of the stonework of door and window surrounds, the most elaborate at the front, the intermediate type forward blocks and other distinctly separate buildings, and a plainer type for corridors and subsidiary buildings. Windows are made in wood in small panes; this provides inconspicuous security as the sashes can only be opened a few inches. The roof is of green Westmorland slate with lead flashings and finials. The entrance hall is impressive with faience tiling to dado height, tessellated flooring with decoration of flowers and geometric patterns, and stained glass windows all set in a space of gracious proportions. In the administrative block the woodwork is of oak, the doors are panelled and the ceilings elaborately plastered. Beyond the entrance hall the wood- work is in pitch pine from northern Russia, and the joinery is of the same high standard. The corridors are all lined by glazed tiles.
The quality of the building drew praise not long after its completion. Dr Daniel Tuke commented: .... it would have been wise to avoid anything in the way of costly embellishment calculated to prejudice the mind of the rate-payer on entering the building. He clarified this point: When visiting this fine asylum I could not help thinking that it may very Possibly be utilized someday as an asylum for the middle and upper classes, Some of whom at present occupy much humbler quarters in private asylums. The building evoked some of the same responses as Hooke's Bethlem in prompting a contrast between the grand appearance of the exterior with the modest provision for inmates. It is sobering to recognise that High Royds Hospital is an example of the most advanced thinking in mental hospital design of the late nineteenth century. The scale of the hospital, the expectation that there would be large numbers of patients who would require minimal care and could contribute to the running of the establishment, the provision of occupation for patients, and the likelihood that many patients would live there until death were dominating influences in the design.
The facilities provided for curative treatments and rehabilitation were minimal. Between the world wars there was increasing optimism about the likelihood of recovery of patients admitted to mental hospitals. This showed itself around the United Kingdom by the building of units for newly admitted patients in which the regimes of patient management were orientated towards the recovery of patients and their discharge from hospital. Most of these units were on the sites of existing mental hospitals and were often called 'neurosis units'. The name implied that the conditions treated were less severe than in the average patient admitted to mental hospitals and that recovery was generally to be expected. Units of this type were built all over the British Isles.
At HRH the building of the new unit began on a peripheral part of the site in 1937 and was opened in 1938. As in the main hospital the unit was in two halves, one for men and one for women, on either side of a central facility which held administrative offices and treatment rooms which were common to the whole unit. The unit was in Modern style with flat roofs, clean rendered walls, metal fittings, verandahs, conservatories, glass bricks and period finishes. Each wing had staff offices and changing rooms near its entrance with a block of bedrooms and bathrooms going off at an angle. The angled wings with verandahs produced a sheltered south facing aspect to each side of the building that allowed patients to sit outside protected from the wind but out of sight of people in the other parts of the building. These features resembled those seen in many houses of the period and gave an atmosphere of modernity and domesticity to the building.
The surrounding area was landscaped to enhance these aspects of the design. When the range of therapies increased in the 1950s, new 'treatment' blocks were added to many of the neurosis units around the country.
At HRH such an extension was planned but not built. The proposed unit would have accommodated outpatient clinics, facilities for investigation such as x-rays suites and pathological laboratories, with accommodation for staff from a range of disciplines.
The development of neurosis units was in many respects a response to a false dawn; mental illness still had a poor outcome. Many of the units came to be absorbed into the general provision of the hospital in whose grounds they were situated and this was the case at HRH.
The closure of HRH in 2003 marked the end of the comprehensive scheme of provision for the mentally ill in the West Riding of Yorkshire which had begun with the planning of Stanley Royd Hospital in 1814, and had led to the building of several major hospitals around the county, and had passed through several distinct phases in the management of mental illness.




.jpg)